Changing the Way We Treat Bladder Cancer
I have been a leader in robotic surgery for bladder cancer since 2006 when I performed my first robotic cystectomy. Since that time, I have been in a leader in advancing this minimally invasive approach to bladder cancer surgery. In leading urologic textbooks like Campbell’s Urology, and in the largest international consortium researching these cutting- edge techniques, I have been recognized for my expertise in bladder cancer care.





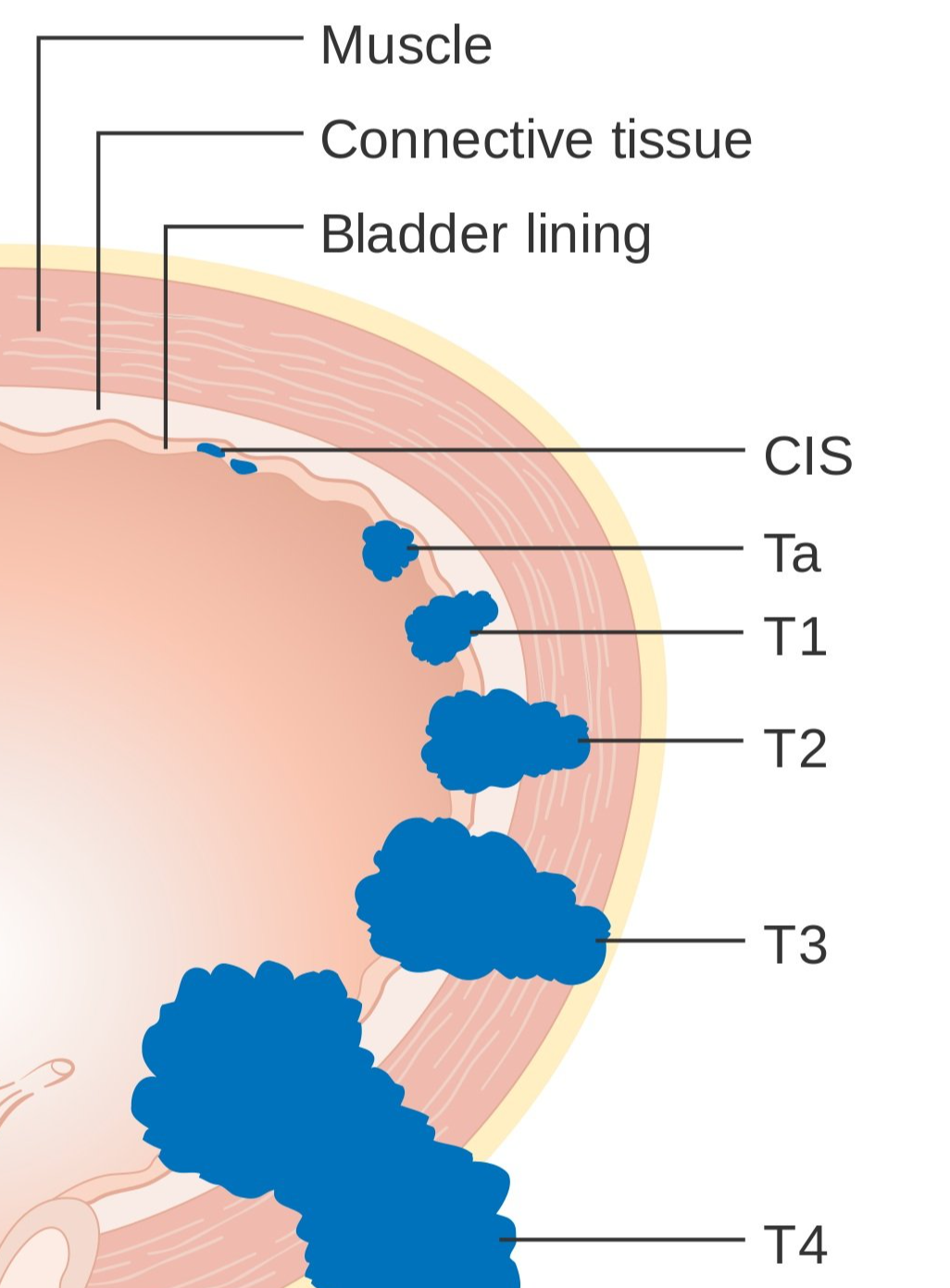
Grade and Stage
Bladder cancer comes in two basic “flavors” known as the GRADE - low grade and high grade. Low grade bladder cancer is very unlikely to spread and is almost always curable. High grade bladder cancer has a higher potential to spread and sometimes necessitate removal of the bladder. Bladder cancer STAGE refers to how deeply the cancer is growing into the wall of the bladder- similar to a plant growing roots into the soil.
Basics
Bladder cancer is typically painless, and usually it is detected when blood is detected in the urine. This can be “microscopic hematuria” - blood in the urine only seen on urine test, not red urine, or “gross hematuria” characterized by red urine. Urologists look into the bladder (called cystoscopy) in order to diagnose bladder cancer. The biggest risk factor for developing bladder cancer is tobacco smoking, either current or in the past.
Cystoscopy
Determining if you have bladder cancer begins by looking in the bladder - a procedure known as cystoscopy - which is performed in the office. If a suspicious area is detected, a cystoscopy is scheduled under anesthesia and the area is removed and biopsied. This is called a “resection” and typically the entire suspicious area/tumor is removed. We refer to this procedure as a “transurethral resection of bladder” - TURB - and the biopsy allows us to determine the GRADE and STAGE